Psychosocial Risk Management in Practice:
A Guide for WHS and HR Leaders
Psychosocial risk management has moved from emerging topic to regulatory expectation.
Across Australia, regulators have clarified that organisations must identify psychosocial hazards, assess the associated risks, and implement effective controls in line with the hierarchy of controls. ISO 45003 reinforces this by embedding psychological health within existing WHS management systems.
For WHS and HR practitioners, the challenge is rarely conceptual.
The challenge is practical:
- How do we conduct a defensible psychosocial risk assessment?
- How do we prioritise hazards accurately?
- How do we avoid defaulting to lower-order controls?
- How do we implement changes in complex, resource-constrained environments?
This article focuses on implementation, not just theory.
Psychosocial Risk Management Considerations
Psychosocial risk management is grounded in structured risk management principles.
ISO 45003 follows a Plan–Do–Check–Act cycle.
Safe Work Australia’s Model Code outlines a four-step process.
In practice, however, two additional stages are often required to ensure effectiveness. Without them, risk assessments frequently fall short.
A practical six-stage process includes:
- Prepare the risk assessment
- Identify psychosocial hazards
- Assess which hazards are risks
- Identify appropriate control measures
- Report findings
- Monitor and review effectiveness
There is nothing radical in this framework. The difference lies in execution.
Step 1: Prepare the Risk Assessment
Preparation is often underestimated.
It requires:
- Defining scope
- Assembling the right team
- Confirming capability and resourcing
- Determining consultation approach
- Securing organisational buy-in
If you do not allocate sufficient time for preparation, the process becomes rushed and superficial.
Preparation determines whether consultation feels genuine. It determines whether leaders are aligned. It determines whether sufficient resources exist to analyse data properly.
Without preparation, a risk assessment becomes a survey exercise.
With preparation, it becomes a change process.
Step 2: Identify Psychosocial Hazards
Identification must use tools designed specifically for psychosocial risk.
Engagement surveys are not psychosocial risk assessments.
They may measure sentiment, but they do not measure exposure, interaction, severity or protective factors.
Identification should include:
- Consultation
- Structured assessment tools
- Review of claims data
- Review of grievance trends
- Examination of operational systems
The key question is: What aspects of work design or management may cause harm?
Not: Are people stressed?
Step 3: Assess Which Hazards Are Risks
Legislation requires consideration of:
- Likelihood of harm
- Severity of harm
- Exposure
However, many assessments fail because they do not evaluate:
- Hazard interaction
- Protective factors
- Existing controls
Hazards rarely operate in isolation. High job demands alone may be manageable.
High job demands + low job control + poor support + trauma exposure becomes significantly more dangerous.
If your methodology does not account for interaction, prioritisation will be inaccurate.
Step 4: Identify Appropriate Control Measures
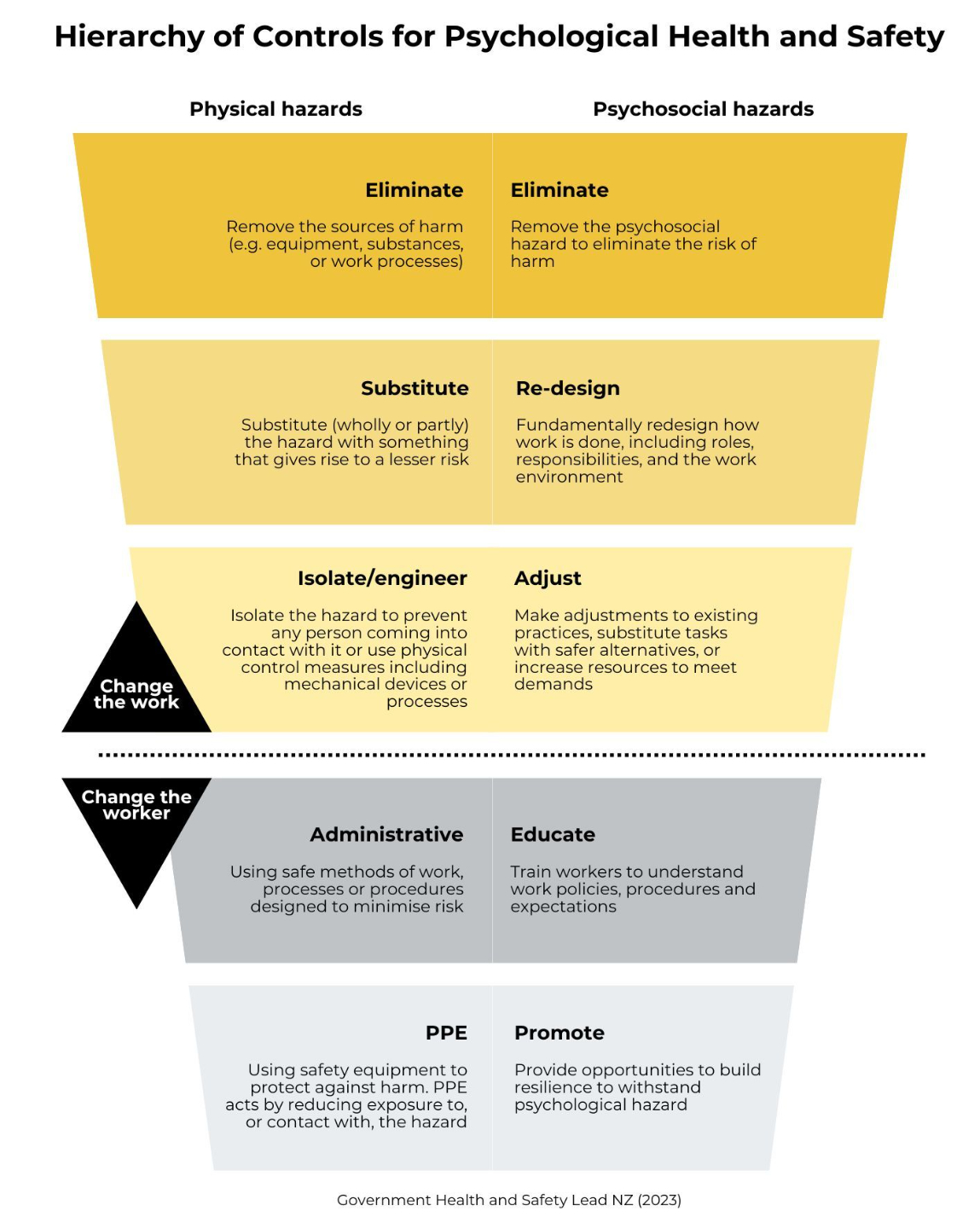
Most jurisdictions now require controls to be mapped on the hierarchy.
Higher-order controls must be prioritised.
Lower-level controls such as training and information are necessary but insufficient on their own.
We return to this in detail below.
Step 5: Report Findings
Organisations frequently fail at this stage.
If you conduct an assessment and do not report findings:
- Staff assume nothing is happening
- Response rates decline in future assessments
- Trust erodes
Step 6: Monitor and Review
Control effectiveness must be reviewed.
This is often neglected because:
- Resources are limited
- Other operational issues arise
But without review, controls drift and become symbolic rather than functional.
Common Barriers to Building Buy-In
Buy-in is not uniform across the organisation. Executives, middle managers and staff require different approaches.
Executives
Executives respond to:
- Risk
- Strategy
- Legal exposure
- Operational continuity
Psychosocial risk must not be framed as a wellness initiative.
Wellness initiatives can be deprioritised when budgets tighten. Risk cannot.
Link psychosocial risk to:
- Existing strategic priorities
- Workforce stability
- Operational risk
- Governance obligations
Middle Managers
Middle managers act as the translation layer.
They often experience initiative fatigue.
Demonstrate how:
- Early identification reduces escalation
- Effective management reduces absence
- Proactive controls reduce operational strain
They must also be resourced appropriately.
Managers who are already overloaded cannot absorb additional responsibility without support.
Staff
Staff require:
- Genuine consultation
- Psychological safety
- Assurance of no negative consequences
- Visible follow-through
Closing the loop is essential.
Without feedback, participation declines.
Scenario-based Learning
Z Correctional Centre is a medium-security facility in regional Western Australia, housing approximately 500 inmates and employing 210 correctional officers plus 60 administrative and support staff. The facility is managed by a state government department.
The centre has faced chronic understaffing for over two years, with a vacancy rate of approximately 22% for custodial officers. To manage the shortfall, remaining officers are regularly required to work double shifts and mandatory overtime, sometimes with fewer than 12 hours between shifts. New recruits receive a shortened induction program (reduced from 12 weeks to 6 weeks) before being deployed on the floor.
18 months ago, a serious assault incident occurred in which a correctional officer was attacked by an inmate and sustained significant physical injuries. Several colleagues witnessed the assault. The officer returned to work after 10 weeks of leave but was placed back into the same unit where the incident occurred, with no phased return-to-work plan and no updated risk assessment for the unit.
A female officer has recently lodged a formal complaint alleging sustained sexual harassment by a senior supervisor over a period of 8 months. She reports that when she raised the issue informally with another supervisor, she was told the behaviour was “just how he is” and to “not make a fuss.” She is now on extended personal leave.
Workers’ compensation claims for PTSD, anxiety, and depression among custodial officers have increased by 85% over the past two years. The average duration of these claims is nearly 3 times the duration of physical injury claims.
The officer who returned after the assault incident has since been diagnosed with PTSD and has been placed on extended leave again. Two other officers who witnessed the incident have also submitted medical certificates citing trauma-related conditions.
Sick leave usage among custodial staff is 40% above the departmental average. Anecdotal reports suggest some officers are self-medicating with alcohol to cope with stress.
The facility’s workplace culture has been described by officers in an internal review as “hypermasculine,” “punitive,” and “us versus them.” Officers report that seeking mental health support is viewed as a sign of weakness and perceived as career-damaging.
Grievance processes are perceived as ineffective. The sexual harassment complaint is the third formal complaint about the same supervisor in two years. Previous complaints were either not investigated or resulted in no action.
Immediate Actions
Immediate priorities included:
- Separating the supervisor subject to harassment complaints
- Initiating an unbiased, trauma-informed investigation
- Providing trauma-informed support to assaulted and witnessing staff
- Reviewing fatigue exposure and rest periods
- Escalating regulatory and legal risk to executive leadership
Short-Term Actions
Short-term priorities included:
- Conducting or commissioning an independent psychosocial risk assessment
- Reviewing the critical incident response process
- Redesigning the return-to-work process
- Ensuring confidential consultation
- Investigating grievance failures
Medium- to Long-Term Actions
Medium-term actions included:
- Addressing staffing shortages as a WHS issue
- Filling the 22% vacancy rate
- Redesigning induction programs
- Building a workplace culture strategy
- Reducing stigma around help-seeking
- Implementing structured peer support
Identifying Psychosocial Hazards in the Scenario
The scenario revealed multiple interacting hazards:
- Exposure to traumatic events
- High job demands
- Low job control
- Fatigue
- Sexual harassment
- Poor organisational justice
- Poor support
- Harmful workplace culture
- Inadequate training
- Violence and aggression
Assessing Risk
A critical question was posed:
Is your methodology accurately assessing and prioritising risk?
Traditional tools such as the People at Work survey are being decommissioned because their methodology does not sufficiently account for:
- Updated hazard frameworks
- Interaction analysis
- Exposure measurement
Risk assessment tools must evolve to reflect regulatory expectations.
Mapping Controls on the Hierarchy
Controls must be mapped appropriately.
Let us support you
Ways we can help:
- Psychosocial Risk Audit - your bespoke dashboard and team of experts
- Train SLT and line managers in psychosocial risk management
- Train staff to understand psychosocial risk and their responsibilities (+ how to regulate stress)
- Wellbeing training that actually works